Radiology
Radiology Review - Shoulder Bankart Lesion

Sport and Exercise Physician | Managing Director
Published
May 4, 2026
Sport and Exercise Physician | Managing Director
Published
May 4, 2026
Shoulder instability is a common but often under-estimated injury in young athletes, particularly those involved in collision sport. While a simple episode may appear straightforward, recurrent instability can lead to progressive structural damage and make later treatment more complex.
In this case, a 20-year-old, right hand dominant semi-professional rugby league player presented with recurring episodes of pain in this right shoulder. He described more than six episodes where he had landed awkwardly on his outstretched arm and had experienced a "dead feeling" in his arm, followed by pain and restricted movement of his shoulder. The most recent episode occurred after a fall onto his chest with his arm abducted and forward flexed.
On examination, the primary findings were a positive anterior apprehension / relocation test, normal axillary nerve function and no evidence of significant glenohumeral joint laxity.
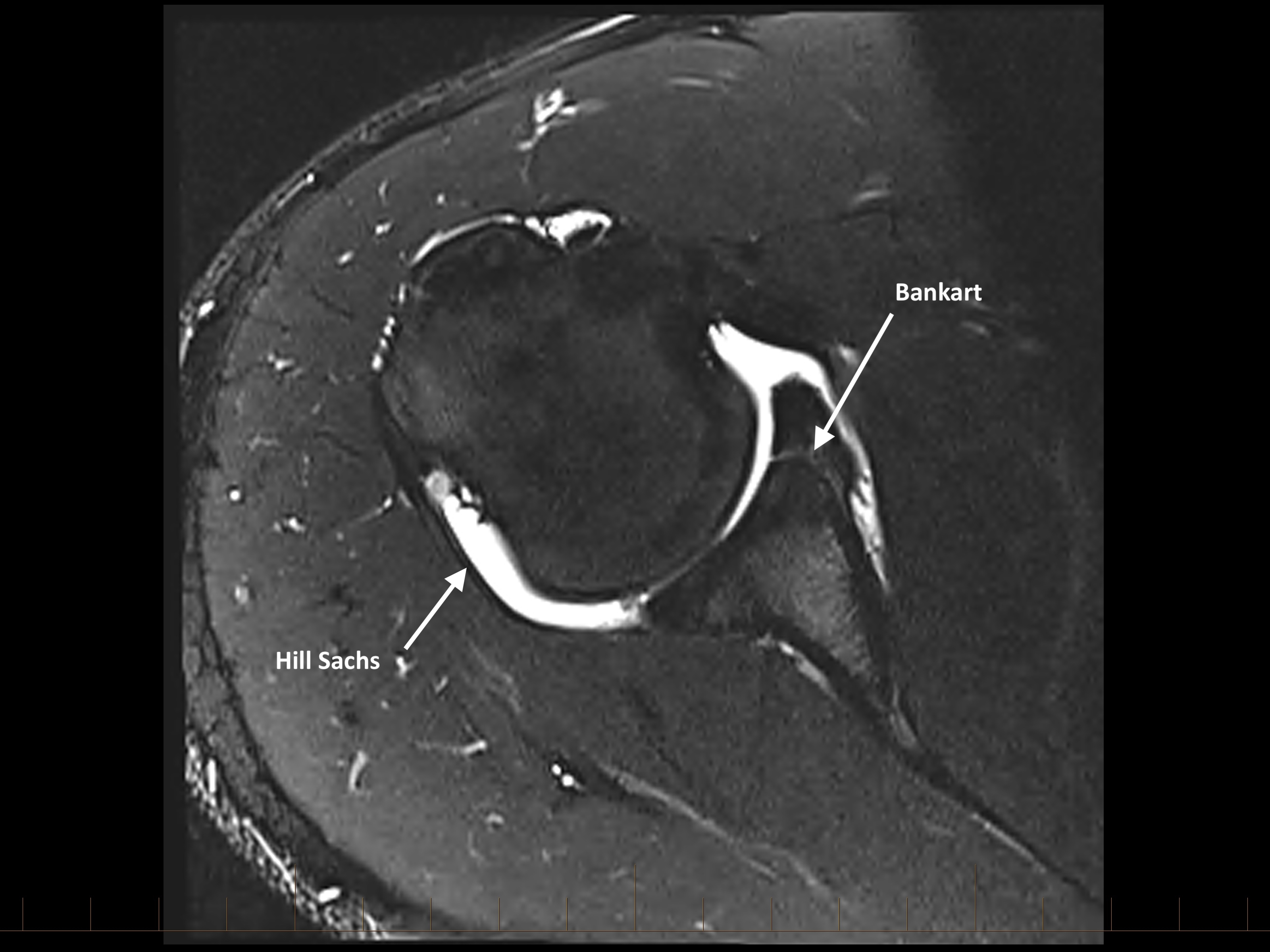
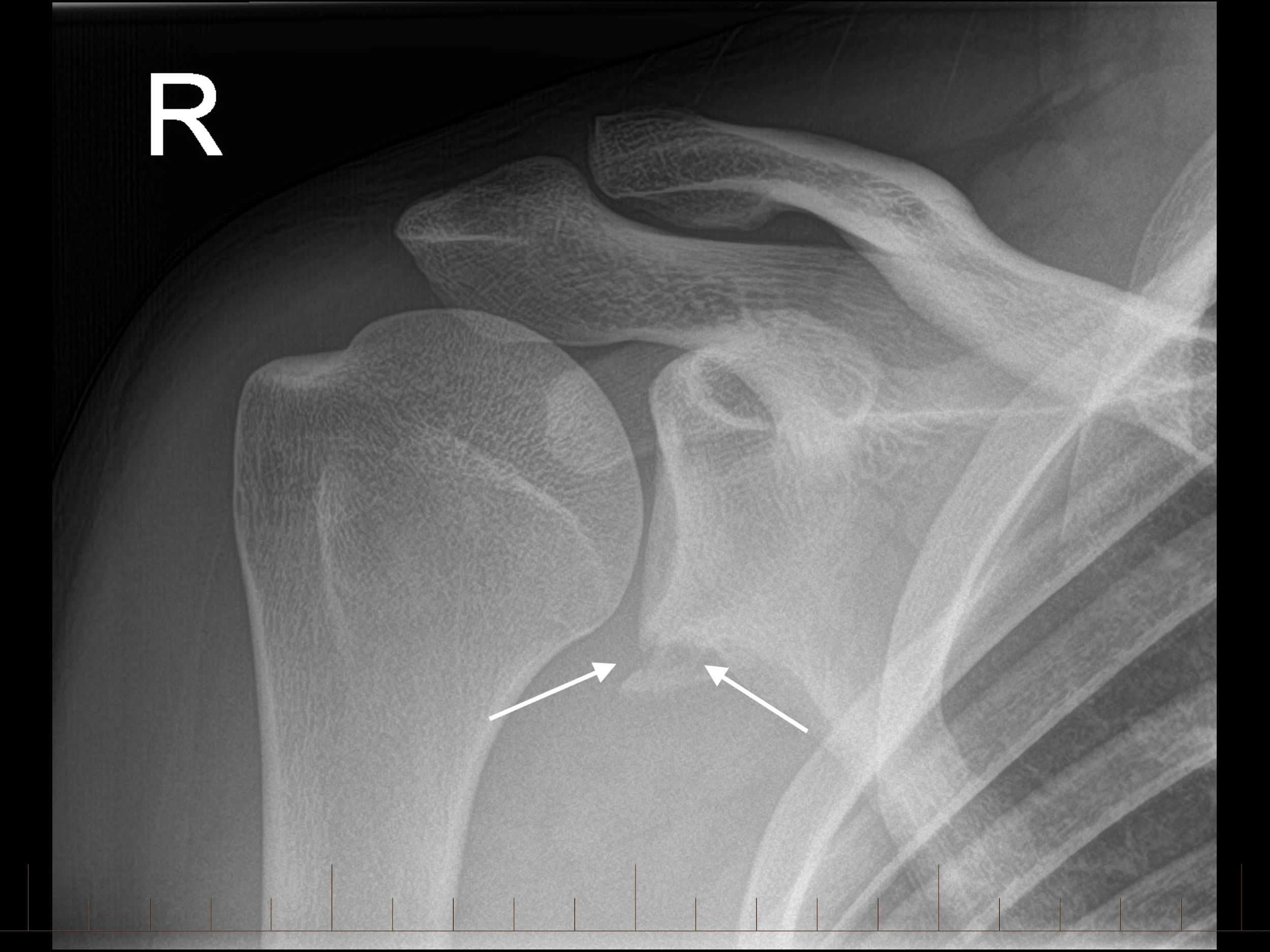
An AP x-ray image shows a fracture involving the inferior glenoid. An MRI arthrogram was conducted with images confirming a large osteo-cartilaginous Bankart lesion. This fracture extends from the 3 o'clock position anteriorly to the 7 o'clock position interiorly (see image 3). There is a small amount of contrast in the defect between the spearted anterior labrum and glenoid.
This player underwent surgical stabilisation due to recurrent instability and the presence of significant glenoid bone loss. An anatomical stabilisation procedure, such as a Bankart repair, has traditionally been considered a gold standard for anterior shoulder instability. However, in collision sport athletes, there is increasing use of bone augmentation procedures such as the Latarjet, given the lower rates of recurrence in higher-risk groups, particularly where bone loss is present. It is important to have a clear discussion with these patients to make sure that they understand that available treatment options and can make an informed decision that best suit their needs. This player made an uneventful recovery and returned to football approximately five months post-operatively.
Shoulder instability is not a benign problem. Most patients have their shoulder reduced in ED and are then given very little information about what to do next. Similarly, patients who sublux (not dislocate their shoulder) often have a delayed diagnosis and have sustained multiple instability episodes before the problem is identified. Recurrence rates are high, particularly in younger patients, those involved in collision sport, and those returning to high-demand or overhead activity. Each subsequent episode of instability risks further structual damage, including progressive glenoid bone loss and enlargement of humeral head defects, which can complicate later management and reduce the likelihood of successful soft tissue repair.
Imaging therefore plays a central role. Beyond confirming the diagnosis, cross-sectional imaging allows quantification of glenoid and characterisation of associated lesions. Bone loss in the range of 20-25% has traditionally been associated with higher failure rates following isolated soft tissue repair. In practice, many young collision athletes are now considered for earlier bone augmentation procedures to reduce recurrence risk and support a more durable return to play.
At Axis, we have started to apply our "acute knee" model to shoulder instability and have started an Acute Shoulder Clinic. Early specialist review, early imaging, and early surgical decision-marking, where appropriate, can alter the trajectory of these injuries. This is particularly relevant for younger, active patients and those involved in contact sport. Our Acute Shoulder Clinic is is designed to provide rapid access to this pathway, with the aim of identifying higher-risk patients early and guiding timely management.