Radiology
Radiology Review - Posterior Ankle Impingement

Sport and Exercise Physician | Managing Director
Published
June 2, 2026
Sport and Exercise Physician | Managing Director
Published
June 2, 2026
Posterior ankle pain in athletes can be easy to mistake for an Achilles tendon problem, especially when symptoms sit close to the tendon and build gradually with training. But sometimes the source is deeper in the back of the ankle.
A 21-year-old professional football player presented with a two-month history of increasing posterior ankle pain. This was initially only present when striking a ball from his 'laces'. It is not present when sprinting and jumping. He has been told he has Achilles tendon problems.
On examination there was pain with the ankle plantar flexion. This was made worse by forced plantar flexion (a posterior thrust test). His ankle and sub-talar range of motion was otherwise normal. He had good power of all ankle movements and no evidence of past instability. He had good power of all ankle movements and no evidence of past instability. The ankle and Achilles examination was otherwise quite unremarkable.
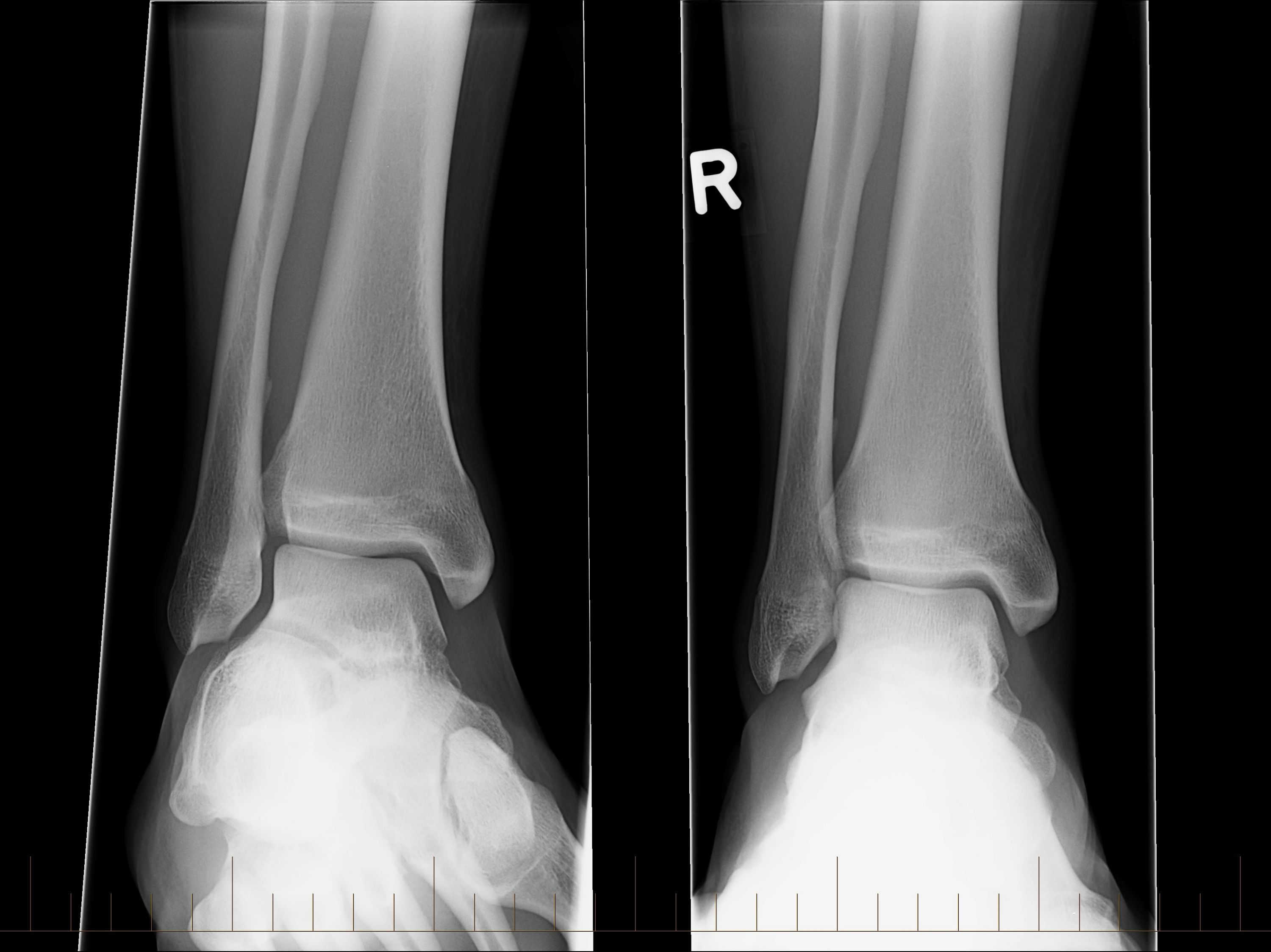
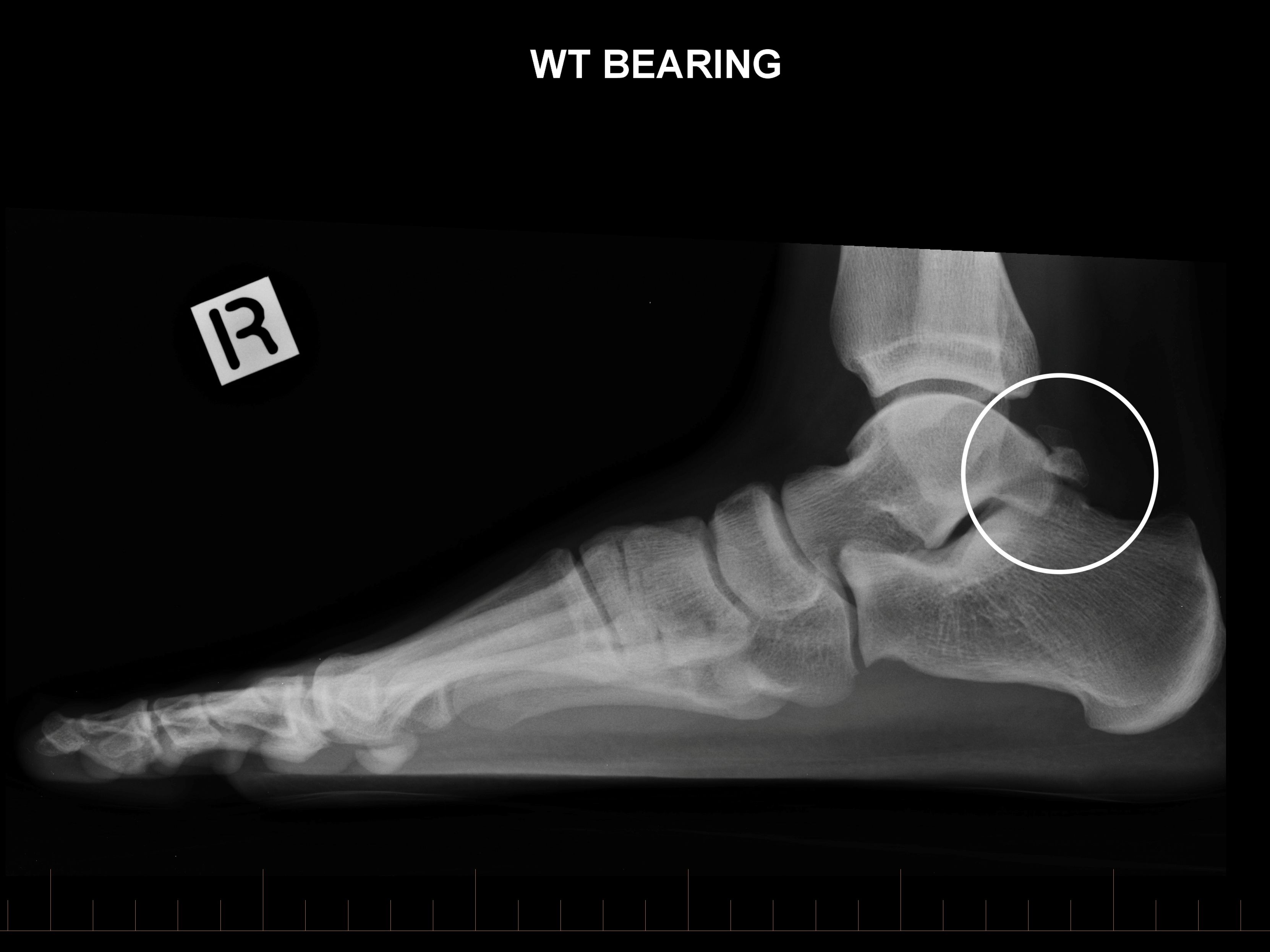
X-ray images, including one taken in a plantar flexed position, show a large os trigonum. An MRI has demonstrated that there is bone oedema within the os trigonum. There is a small amount of subchondral cyst formation and reactive change in the posterior process of the talus adjacent to the synchondrosis. The appearance suggests an unstable os trigonum. The os is also quite large measuring approximately 12 x 12 x 7 mm.
This player was diagnosed with posterior impingement of the ankle. This was initially managed with time, physiotherapy and taping to limit ankle plantar flexion. This was followed by a transient improvement with a corticosteroid injection into the posterior ankle. Unfortunately, the player's symptoms returned, and surgery was eventually required to excise the os trigonum. This was done at the end of their competitive season. They were able to return to all normal activity a little after three months post-surgery.
Consider a possible diagnosis of posterior impingement in all athletes who present with posterior ankle and Achilles tendon region pain. Impingement is generally easy to identify as the player's posterior ankle symptoms will be reliably reproduced by forced plantar flexion. I generally do this with the patient lying prone and their knee flexed to 90 degrees. In this position I can make sure that I am able to fully plantarflex the ankle and stabilise the midfoot. I can also palpate the posterior ankle and Achilles tendon, which is also important. Once you have made a clinical diagnosis and of posterior impingement it is important to consider why this has occurred. This may be due to bony or soft tissue causes (or both). Posterior impingement can have a variety of causes. A prominent posterior process of the talus or os trigonum (as in this case) may predispose a player to developing this condition. Soft tissue causes of impingement include synovial hypertrophy, capsular injury, ligament injury and flexor hallucis longus (FHL) tenosynovitis or tendinitis. Some of these problems occur after an acute ankle injury, for example to the lateral ligaments. In this situation as an athlete's acute symptoms settle, they will generally report awareness of pain in the back of the ankle as they return to training.
In very general terms impingement often resolves with avoidance of aggravating activity. Taping or bracing to prevent terminal plantar flexion (or dorsiflexion when there is anterior impingement) can allow a player to remain active. Oral NSAIDs can also be helpful. Steroid injections can provide very dramatic relief of symptoms if these other interventions fail but unfortunately often only give short-term relief where there is structural cause for the impingement (as there was in this case). When the symptoms are refractory to treatment, arthroscopic debridement can give a good result.